Nail surgery: a personal perspective.
I've recently had nail surgery to my right great toe, so I thought it would be good to record as a blog and look at my personal experience of the procedure.
You can check out the full blog post here.
Minor surgical procedures for problematic, ingrowing, thickened or fungal nails can be provided at Walk. If you have any questions, comments, or wish to enquire about an appointment then please get in touch.
Tel: 01562 515661
Mobile: 077 666 888 29
Email: contact@walkfootcare.co.uk
www.walkfootcare.co.uk
Love Feet, Love Life...
For many chiropodists and podiatrists the main type of the work they do involves the use of instruments to treat hard skin or nails.These instruments can be broadly placed into three different categories: single use (i.e. used once and disposed of), single patient use/patient held (i.e. instruments used on a single patient multiple times and looked after by the patient) or reusable (decontaminated between patients).Each system has its pros and cons and the one the podiatrist chooses will be based on many considerations including financial, storage and moral/ethical viewpoints.At Walk we have chosen to use reusable instruments because we feel that these offer the best solution for our patients and also for us as practitioners, being of superb quality and longevity, reducing the chance of repetitive strain injuries and having a smaller impact on the environment by reducing waste.All of our instruments undergo a full process of decontamination which is defined as “the combination of processes which includes cleaning, disinfection and sterilization to render a reusable item safe for further use.” (Society of Chiropodists and Podiatrists, 2009).We want to ensure that the instruments we use are safe and fit for the intended purpose without putting our patients at risk. To that end, we use the following process to decontaminate our instruments:1. Dirty instruments are manually cleaned using a brush and cleaning solution in warm water.2. Instruments are transferred for an ultrasonic cleaner to remove small and difficult to remove pieces of debris.3. Instruments are then rinsed in a dedicated sink to remove debris and the cleaning solution.4. Once rinsed, instruments are then placed in an autoclave and sterilised for a total of three minutes at a temperature between 134 and 137 degrees centigrade.While this process can be completed in the clinical room, it is recommended that a separate room is used to safeguard patients and clinicians. At Walk we use room adjacent to the clinical room for decontamination.Our autoclave meets the Pressure Systems Safety Regulations (2000) and is examined annually by a competent person to ensure that the machine continues to meet these requirements and the results of these tests are available to any patient upon request.The autoclave we use has a printer attached that provides a breakdown of the sterilising cycle showing the temperature during the three-minute programme. This is checked by the podiatrist upon completion of the cycle and the printout stored in a separate folder and countersigned for our records. This ensures that the process we use is transparent and can be traced. Again, patients can freely examine these records upon request.Each pack is then marked with the date of sterilisation and initialled by the clinician who has sterilised the instruments. If the instruments are not used within a set period of time then they undergo the decontamination process again.So there’s a lot that goes into making sure that the instruments we use are sterile and free from infection, but we’re happy that this is the best process for us and represents the greatest safety for our patients.If you have any questions about our decontamination process or would like to book an appointment then please get in touch on 01562 515661 or 077 666 888 29.References:Society of Chiropodists and Podiatrists (2009) Standards for the decontamination of reusable podiatry instruments in primary care. [Online: http://www.pebblepad.co.uk/scpod/download.aspx?oid=14032&useroid=0&action=view] [Accessed: 19/05/2013]
I have a friend and colleague (a podiatrist) who has recently managed to fracture the base of her fifth metatarsal. So I thought it would be useful to look fractures in this area and look at how they present, are diagnosed and are treated.She has kindly sent me pictures of her foot prior to diagnosis of the fracture, in the walking boot and also the x-ray itself, which shows the area damaged. She has also said she is happy for me to write about it here as a case study.A fracture can simply be described as a break in the continuity of the bone. They can result in damage across the whole of the bone, or part of the bone, such as in a Greenstick fracture.Fractures to the metatarsal bones are one of the most common injuries to the foot with up to 70% involving the fifth metatarsal (Polzer et al, 2012), the metatarsal near to the outside edge of the foot.Commonly an individual will present with pain to the foot sustained after a traumatic event such as an inversion injury to the ankle. For the most part, this kind of injury will result in a sprain to the ligaments on the outside of the foot and ankle, although at times it can be more sinister.SymptomsThe main symptoms that patients report following an injury is pain, swelling, bruising and inability to weight bear. In some severe injuries a wound may be present over the site of injury and bone could be seen – in this case this is a serious emergency and a rapid trip to the Emergency Department (ED) is recommended! The symptoms above are not restricted to fractures; in fact many soft tissue injuries present with similar features. An x-ray is the only way in the early stages that you can definitively identify a fracture. So how do you find out who needs an x-ray and who doesn’t?The Ottawa Ankle Rules (OAR)The OAR is a simple test to examine who needs an x-ray in the ED. After all x-rays use radiation so you don’t want to go and irradiate people recklessly. They were first used in 1992 to try to reduce the cost of radiology and also the time that patients spent waiting in the ED. Tenderness in predefined locations with the inability to bear weight is considered a positive finding and an –x-ray is ordered. The test is geared towards a high sensitivity – essentially this means that a negative result (i.e. no pain and can bear weight) means no x-ray thus saving time in the ED and financial resources for tests that may not be needed.The use of the OAR may explain why in the past an individual had an injury but the doctor decided not to x-ray.So I have a fracture? What next?The treatment will depend upon the location, severity and displacement (how lined-up it is) of the fracture, combined with the patient’s symptoms. In the initial stages patients may be non-weight bearing in either a cast, walking boot or an elasticated bandage. With regards to weight bearing, authors differ on their approach with some recommending complete non-weight bearing for 8 weeks (Hopton & Harris, 2010) while others suggested weight bearing as tolerated (Polzeret al, 2012). The treatment offered might well depend upon the clinical experience of the individual coupled with the severity of the injury.In the case of my colleague, she was initially treated with a plaster of Paris “backslab” which sits upon the back of the leg and the sole of the foot to protect the area from further injury. This is a temporary cast and has been replaced with a removable boot that allows her to bear weight when ready. It also allows her to keep the foot clean and maintain her hygiene; something that a plaster cast cannot allow.Will I need an operation?In some cases an operation may be needed but this is normally limited to severe fractures or those that fail to heal with conservative and functional measures. Kerkhoffs et al (2011) looked at surgical treatment for avulsion fractures in athletes and non-athletes and found that those who had surgery healed quicker and returned to sports sooner. Although they did say their treatment approach with a simple lined-up fracture was to use conservative and functional measures.How long will it take to heal?The research seems pretty consistent here and found that on average the fracture shows signs of healing on x-ray within 6-12 weeks. SummarySo it seems that fractures to the 5th metatarsal are common and if uncomplicated can be treated fairly simply with control of individual patient symptoms. If all goes well, most will heal between 6-12 weeks.I will try to keep you updated with my friend’s progress as she recovers from her injury.Fractures in the acute stages are not something which we can deal at Walk other than recommending further examination; however, once healing has occurred and you return to your normal level of activity we can aid rehabilitation. Fractures and the immobilisation of the the foot and leg can lead to functional problems that we are well placed to treat using soft tissue and joint mobilisation. Why not get in touch to find out more?Tel: 01562 51 56 61Mobile: 077 666 888 29Email: contact@walkfootcare.co.ukReferences:POLZER H, POLZER S, MUTSCHLER W & PRALL WC (2012) Acute fractures of the proximal fifth metatarsal bone: Development of classification and treatment recommendations based on current evidence. Injury. 43:1626-1632.HOPTON BP & HARRIS NJ (2010) Fractures of the foot and ankle. Orthopaedic Surgery: Lower Limb. 28(10): 502-507.KERKHOFFS GM, VERSTEEGH VE, SIEREVELT IN, KLOEN P & VAN DIJK, CN (2012) Treatment of proximal metatarsal V fractures in athletes and non-athletes. British Journal of Sports Medicine. 46:644-648.
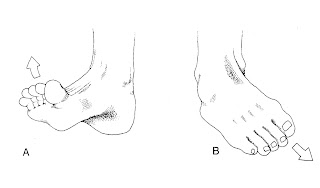
This article was first published in Ryding2Health Magazine in 2011 and is the first time it has been on my blog. I've made some small edits which I never had the chance to do first time round, so hopefully it reads better!As always please feel free to comment.Pronation is a subject close to many a podiatrist’s heart and traditionally the focus of treatment in many biomechanical pathologies. Patients regularly tell me that they “pronate too much” or that they “overpronate” and that their feet are “flat”. In my experience, the main group of patients who consider pronation more than many other groups are runners. I suppose the question is; is pronation really a bad thing?Let’s begin with identifying exactly what pronation is, and when it occurs.Pronation is a three-dimensional movement occurring at the subtalar joint in the foot. Sounds simple enough, but don’t be lulled into a false sense of security; podiatrists undertake three years of study to understand it and relate it to an individual’s biomechanics and that’s just the beginning!Now before I get inundated with corrections, I know that pronation also occurs in the arm too; but I’m a podiatrist and I only really get to play with feet and legs. For more information on the arm you’ll need to talk to your local physiotherapist.When pronation occurs, it allows the forefoot to abduct (move away from the midline of the body) upon the rearfoot, dorsiflex (or lift upwards) in relation to the rearfoot, and evert or flatten the arch of the foot. The overall view of a foot in pronation is that of a “flat foot”. The opposite of pronation is supination and when the foot becomes more supinated it takes on a “high arched” profile.The diagram shown above (taken from Michaud (1997)) shows both pronation and supination movements.Now, both of these movements are essential and we use both as part of normal “gait". As a general rule, when walking the foot strikes the ground in it’s supinated form, becomes pronated to shock absorb the body forces upon the ground, and the becomes supinated again prior to lifting of the ground so as to provide a rigid leverage force to move to the next step.So is pronation bad?On the whole pronation is not a bad thing; it’s a necessary movement required for normal ambulation, be it walking, running or your activity of choice. Interestingly there have been many studies examining the link between pronation and injury and most show that there is little relationship between injury and pronation (those which do show a link are pretty weak). Pronation is key in providing shock absorption as the foot makes contact with the ground and then body-mass continues in a downward direction. These movements require a very complex interplay between joints, ligaments, muscles and the forces acting upon these structures.Often this will become imbalanced when the forces cannot be controlled or opposed by the body, leading to compensation and then injury.My role is to examine areas of compensation and injury and identify the causative factor. This involves looking at the forces acting upon the foot from internally (muscles, ligaments, joints, etc) and externally (footwear, the supporting surface, orthotics) to ensure that a balance is struck. There are a number of tests that we use clinically to look at how easy (or hard) it is to move the foot from a maximally pronated position to a supinated position.These forces change when different activities are undertaken; running, has much greater forces affecting the foot and leg in comparison to walking.When it comes to pronation, the movement isn’t such a bad thing, it’s the forces that hurt and cause damage. My treatment involves the reduction of these pathological forces and this can involve the use of exercises, footwear, orthotics and mobilisation. So what about running shoes? Okay, you were always going to ask. Running shoe design, prescription and personal choice is based on the idea of levels of pronation. And while this is flawed it is really all we have. However, this will change in the future with some interesting and potentially game changing designs coming from Asics and other companies.A very experienced and knowledgeable Sports Podiatry colleague, Ian Griffiths, wrote an excellent blog regarding running shoe prescription and I would urge you all to go and have a look. It surmises the issues and research perfectly. You can find the blog post here http://www.ransacker.co.uk/running-shoes/goings-on/what-running-shoes-should-you-wear-the-myths-busted/.This article is a designed to be a quick look at a very complex subject and in essence doesn’t cover everything. Contemporary research is continuing to challenge current and past dogma leading ultimately to a greater understanding of lower limb biomechanics. Personally, I think it's a very exciting time for anyone working in biomechanics.ReferencesMichaud, T (1997) Foot Orthoses and other forms of conservative foot care. Newton, Massachusetts.
 |
| Podiatrist Dave James |
Dave James had the pleasure of visiting the Pound Green stroke group today to provide a talk on common foot problems and how they are managed.The presentation covered a number of subjects including skin and nail problems, diabetes, surgery, verrucae and biomechanics. The group asked some excellent questions and happily discussed their own issues and experience. They also enjoyed the pictures of foot problems.The session finished with the opportunity for group members to have a foot examination and get some advice from Dave.Many thanks for Brian and the group for inviting Walk to provide a talk. We look forward to talking to the Bewdley group in the next few weeks.If you would like a podiatrist from Walk to visit your group to provide education on foot health then please get in touch on 077 666 888 29 or contact@walkfootcare.co.uk.
Foot pain is common and of all the locations for foot pain that I see as a podiatrist, the most common has to be pain in the heel and pain in the arch.Perform a search on the internet for heel pain and the top "hit" will usually be related to a condition called plantar fasciitis. Much debate exists on exactly what plantar fasciitis is and whether it is truly related to inflammation. That debate is one which will continue as we continue to understand the condition more but for now let's keep it simple.Plantar fasciitis can be viewed as an overuse injury to the origin of the plantar fascia related to excessive stress or biomechanics abnormalities of the foot (Healey and Chen, 2010). The plantar fascia is a tight band of connective tissue situated on the bottom of the foot running from the calcaneus (heel bone) to the toes. It is important because it helps to support the structures of the foot during ambulation, helping you to progress from the moment your foot strikes the ground to the moment you bend your big toe and lift your foot. The pain of plantar fasciitis affects this process, making ambulation less energy efficient and potentially leading to problems elsewhere in the body.With plantar fasciitis, patients will often report a pain in the heel, present after rest (for example first thing in the morning) which then eases upon walking. Generally activity is limited and for some it can be a debilitating problem. A detailed patient history can often identify a traumatic event or a change in shoes which has led to the onset of the symptoms.Plantar fasciitis is common (Goff and Crawford, 2011) with approximately 10% of the population suffering (Crawford and Thompson, 2008). So how do we treat it?Plantar fasciitis is on the whole self limiting - it will go away on its own. That's the good news, but if it goes on its own, why do people come to the clinic? How long it takes to resolve will differ between individuals but in some cases it could be upwards of 12 months and that is why treatment it sought.The mainstay of treatment is stretches to the calf muscles, the muscles on the bottom of the leg below the knee and the plantar fascia itself. Stretches have been shown to provide symptom reduction and improve function.There is also evidence for using orthoses or shoe inserts in the early stages of plantar fasciitis to help reduce pathological forces which act upon the foot, reducing compensation from biomechanical problems.At Walk our podiatrists can fully assess the heel pain examining your biomechanics to provide the best solution for you. We will provide advice on stretching, footwear and if required issue you with a set of foot orthoses.To complement this we can also provide foot joint and soft tissue mobilisation techniques to the foot and ankle which helps with the rehabilitation of the area.There are lots of causes of heel pain with not all of these originating in the foot. Pain can be referred from other structures such as the lower back which cause pain in the foot. This is why it is important to see a professional to diagnose the problem and provide an evidence based management plan.If you have any problems with your feet and legs, or questions and queries regarding your foot health then please contact us on 077 666 888 29 or 01562 51 56 61. You can also contact us via email - contact@walkfootcare.co.uk.References:Healey, K. and Chen, K. 2010. Plantar Faciitis: Current Diagnostic Modalities and Treatments. Clin Podiatr Med Surg 27, pp. 369–380.Goff, J.D. and Crawford, R. 2011. Diagnosis and treatment of plantar fasciitis. American family physician 84(6), pp. 676–82.Crawford and Thomson 2010. Interventions for treating plantar heel pain (Review). The Cochrane Library (1).





